Suffering from polio in his teens propelled Dr. Vladimir Janda into a medical career that ultimately resulted in his “crossed syndromes” of muscle imbalance. Globally recognized, Janda’s crossed syndromes have come to play an integral role in the management of chronic musculoskeletal pain.
His crossed syndromes explain the type of muscle imbalances one can expect to experience when afflicted with a disruption in sensorimotor functioning, imbalances that can lead to more severe issues down the line.
Janda Approach to Chronic Musculoskeletal Pain
Janda Approach to Chronic Musculoskeletal Pain
Janda came up with his theories by taking the functional approach to musculoskeletal medicine. The functional approach looks at the function of all systems and processes throughout the entire body, not just the localized site of the pain. As he found through research, clinical observations and his own physical suffering, the site of the pain is not always the cause of the pain, especially when it comes to musculoskeletal issues.
Janda’s approach is based in the idea that the musculoskeletal system and the central nervous system are interdependent, forming the sensorimotor system. A change in one part of the sensorimotor system will lead to a change in another part of the system as the body attempts to maintain internal stability, or homeostasis.
Changes in the sensorimotor system often show up in the muscular system. If chronic pain stems from the central nervous system, the patterns of muscle imbalance that accompany the pain are often caused by neurological, rather than structural, changes. Janda found the patterns of imbalance were predictable and would inevitably spread throughout the muscular system. That predictability is where his crossed syndromes come into play.
Tonic vs. Phasic Muscles
Tonic vs. Phasic Muscles
Janda found muscles generally fell into one of two groups: tonic or phasic. Tonic muscles are those involved in rhythmic or repetitive activity and activated with flexor activity. Phasic muscles are the “extensors” which work eccentrically against the force of gravity. Tonic muscles tend to tighten or shorten while phasic muscles are prone to inhibition or weakness. The categories work as a guide to predict muscle reactions, although exceptions can occur.
Upper Crossed Syndrome (UCS)
Upper Crossed Syndrome (UCS)
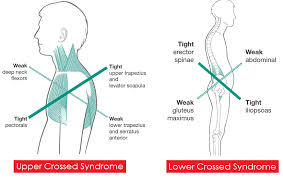
Also known as cervical crossed syndrome, UCS results in the chronic tightening of certain upper-body muscles and chronic weakening of others. The zones of tightening and weakness alternate, forming an “X” pattern.
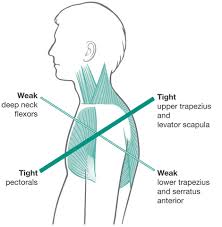
Tightening of:
-
Upper trapezius
-
Levator scauplae
-
Sternocleidomastoid
-
Pectoralis muscles
Upper trapezius
Upper trapezius
Levator scauplae
Levator scauplae
Sternocleidomastoid
Sternocleidomastoid
Pectoralis muscles
Pectoralis muscles
Weakening of:
-
Deep cervical flexors
-
Lower trapezius
-
Serratus anterior
Deep cervical flexors
Deep cervical flexors
Lower trapezius
Lower trapezius
Serratus anterior
Serratus anterior
Lower Crossed Syndrome (LCS)
her responseright here
Lower Crossed Syndrome (LCS)
Also called pelvic crossed syndrome, LCS results in the chronic tightening and weakening of specific lower-body muscles, also forming an “X” pattern.
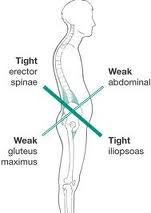
Tightening of:
-
Thoraco-lumbar extensors
-
Rectus femoris
-
Iliopsoas
Thoraco-lumbar extensors
Thoraco-lumbar extensors
Rectus femoris
Rectus femoris
Iliopsoas
Iliopsoas
Weakening of:
-
Abdominals
-
Gluteal muscles
Abdominals
Abdominals
Gluteal muscles
Gluteal muscles
Janda’s syndromes can help clinicians predict patterns of weakness and tightness, with the changes in muscular tone creating a muscle imbalance that can ultimately lead to compromised posture and dysfunction in movement. The movement dysfunctions and imbalances can eventually result in joint degeneration if they are affecting joint surfaces. Being aware of his syndromes can save time, effort and resources when it comes to determining and treating the root cause of dysfunction and pain.
REFERENCES:
REFERENCES:
Morris CE, Greenman PE, Bullock MI, Basmajian JV, Kobesova A. Vladimir Janda, MD, DSc: Tribute to a Master of Rehabilitation. Spine. 2006;31(9): 1060–1064.
Morris CE, Greenman PE, Bullock MI, Basmajian JV, Kobesova A. Vladimir Janda, MD, DSc: Tribute to a Master of Rehabilitation. Spine. 2006;31(9): 1060–1064.
Spine.
Page P, Frank C. The Janda approach to chronic musculoskeletal pain emphasizes muscle function. Adv Phys Ther Rehab Med. 2003;12(1):27.
Page P, Frank C. The Janda approach to chronic musculoskeletal pain emphasizes muscle function. Adv Phys Ther Rehab Med. 2003;12(1):27.
Adv Phys Ther Rehab Med.